Estimated Read Time: 7 minutes
Key Takeaways (Quick Summary):
• High Failure Rates: 49% of all diabetic foot ulcers fail to heal with traditional care, and 50% of venous leg ulcers have been present for at least nine months upon initial presentation [1][2].
• Emergent Action Required: Diabetic foot ulcers failing to achieve at least a 53% area reduction after four weeks of traditional treatment only have a 9% chance of healing by the 12-week mark [3].
• Holistic Evaluation: Outpatient wound center patients average eight comorbid conditions, necessitating comprehensive systemic management alongside local wound care [4].
• Biofilm Management: Biofilm begins to reform within 24 hours of sharp debridement [13] and re-establishes within three days [14], requiring frequent intervention.
• Gold Standard Offloading: Total contact casting (TCC) heals up to 90% of nonischemic diabetic foot ulcers [8] in an average of 34 days [7].
• Therapeutic Compression: Healing venous leg disease mandates graduated compression at an initial pressure of 30-40 mmHg to collapse the targeted vessels [25][26].
Why are chronic lower extremity ulcers considered a dire and emergent clinical pathology?
Chronic ulcers of the lower extremity are among the most devastating pathologies treated by wound care specialists. Chronic ulcers carry with them high morbidity and mortality, along with a high rate of failure to heal.
For example, 49% of all diabetic foot ulcers fail to heal despite traditional good ulcer care [1] and 50% of venous leg ulcers have been present for at least nine months [2] on initial presentation.
Chronic ulcers present not only a dire situation, but also an emergent one. This is evidenced by the fact that diabetic foot ulcers whose percentage area reduction is not at least 53% after four weeks of traditional treatment only go on to heal by the 12-week mark 9% of the time [3]. These foreboding statistics are among the many that support the need for advanced treatment options and evidence-based decisions when caring for chronic ulcers.
How do comorbidities affect the development and chronicity of lower extremity ulcers?
 Before making treatment decisions regarding the ulcer itself, it is important to evaluate comorbid conditions that may have contributed to the development of the ulcer and/or its chronicity. This can be daunting when considering data from the U.S. Wound Registry indicates that patients seen in outpatient wound centers have an average of eight comorbid conditions [4]. However, a thorough history taken in a methodical fashion should allow for the detection of all potentially complicating factors. These potential comorbidities include malnutrition, immobility, obesity, cardiopulmonary disease, poor glycemic control in patients with diabetes, peripheral arterial disease, venous insufficiency, immunodeficiency, advanced age, neuropathic conditions, metabolic disorders, hematologic disorders, neoplastic conditions, local and systemic infection, tobacco use, and psychosocial issues [4]. Upon detection, it is important that any of these be addressed and managed as best as possible. This may require referral to another specialist. Ignoring a contributing systemic condition may render any local care futile.
Before making treatment decisions regarding the ulcer itself, it is important to evaluate comorbid conditions that may have contributed to the development of the ulcer and/or its chronicity. This can be daunting when considering data from the U.S. Wound Registry indicates that patients seen in outpatient wound centers have an average of eight comorbid conditions [4]. However, a thorough history taken in a methodical fashion should allow for the detection of all potentially complicating factors. These potential comorbidities include malnutrition, immobility, obesity, cardiopulmonary disease, poor glycemic control in patients with diabetes, peripheral arterial disease, venous insufficiency, immunodeficiency, advanced age, neuropathic conditions, metabolic disorders, hematologic disorders, neoplastic conditions, local and systemic infection, tobacco use, and psychosocial issues [4]. Upon detection, it is important that any of these be addressed and managed as best as possible. This may require referral to another specialist. Ignoring a contributing systemic condition may render any local care futile.
What characteristics must be documented during a consistent ulcer evaluation?
Consistent evaluation and documentation of ulcer characteristics is an essential component of chronic ulcer management. This allows for consistency between different providers and tracking of progress. It is also important for risk management. Clinicians should document the location of the ulcer; the ulcer length, width, and depth; drainage (quantity, color, and type); color of the ulcer bed and surrounding tissue; the absence or presence of necrotic tissue; vascularity; texture of the ulcer bed and surrounding tissue; temperature surrounding the ulcer; general condition of the ulcer bed and surrounding tissue; and the presence or absence of undermining/tunneling, and if present, orientation and extent.
What is the clinical distinction between contamination, colonization, and infection?
Contamination, colonization, and infection are all states that wound care providers should be familiar with. Contamination indicates the presence of non-replicating organisms in the ulcer bed. All chronic ulcers are contaminated [5]. It is for this reason that superficial culture swabs cannot be relied upon to determine if an ulcer is infected, nor should they be used to identify causative organisms in the presence of infection [6]. Colonization indicates the presence of replicating organisms that are not causing tissue damage. This usually represents skin flora. Infection sets in when these replicating organisms begin to cause tissue damage. It is best to culture an ulcer only when infection is suspected [7]. This helps to avoid false positives and overutilization of antimicrobials. When culture is warranted, it is best to be performed, when possible, as a deep tissue culture under sterile conditions. When infection is confirmed, antimicrobial therapy should be targeted based on culture and sensitivity reports.
What are the most effective offloading methods for plantar foot ulcers?
Total contact casting (TCC) is the gold standard [8]. The evaluation of the ulcer should include evaluation for the need to offload, which includes a gait analysis and checking for any underlying bony prominences. Plantar foot ulcers can be especially stubborn when not properly offloaded. There are many offloading options with wildly different rates of efficacy. A rigid, flat-bottom postsurgical shoe is intended to accommodate bulky postsurgical dressings and was never intended to serve as an offloading device. There is no statistically significant data to suggest that a rigid, flat-bottom postsurgical shoe offloads the plantar foot more than any standard shoe. The same is true for the offloading abilities of forefoot and rearfoot wedge shoes. True offloading is best achieved with a total contact cast.
Total contact casting heals up to 90% of nonischemic diabetic foot ulcers [8]. Not only is total contact casting extraordinarily impactful in healing diabetic foot ulcers, the time to healing is fast at an average of just 34 days [7].
Removable cast boots have proven to offload just as effectively as total contact casts [9]. However, removable cast boots are flawed because they can be removed by patients, which can occur as often as 72% of the time [10]. Irremovable cast boots offload just as effectively as total contact casts with equal rates of ulcer healing [8].
Which methods of debridement are indicated for chronic ulcers?

Debridement is indicated for most chronic ulcers to remove necrotic and/or non-viable tissue, which can serve as a medium for infection, acts as a barrier to healing, contributes to the formation of matrix metalloproteinases, and increases the bioburden of the ulcer bed. There are multiple forms of debridement. Biosurgical debridement refers to maggot or larval therapy, a selective form where larvae liquefy and ingest necrotic tissue via proteolytic enzymes. Enzymatic debridement refers to the use of exogenous enzyme(s) to cleave the strands of collagen that anchor necrotic tissue to the bed of the ulcer. Whereas enzymatic debridement relies on exogenous enzymes, autolytic debridement enlists the body’s own endogenous enzymes, typically a slower process facilitated by surgical dressings like hydrogel and hydrocolloid that maintain moisture. Chemical debridement usually refers to the use of silver nitrate to address hypergranulation tissue. Mechanical debridement includes irrigation, pulse lavage, whirlpool, and scrubbing, though wet-to-dry or moist-to-dry dressings are considered substandard and should not be used [11]. Low frequency ultrasound-assisted debridement may also be employed in noncontact or contact forms.
How often should sharp debridement be performed to prevent biofilm reformation?
Sharp debridement should be performed frequently because chronic ulcers demonstrate better healing with more frequent debridements [12]. Sharp debridement may be performed with scissors, forceps, lasers, hydrosurgical options, curettes, and/or scalpels. The frequency with which sharp debridements are performed should be based on peer-reviewed literature.
Peer-reviewed literature [12] establishes that this is likely due to the fact that biofilm returns quickly after sharp debridement, beginning to reform within 24 hours [13] and re-establishing itself within three days [14].
Not only should sharp debridement be performed frequently, but there are also multiple studies that suggest ulcer progression is improved when sharp debridement is combined with enzymatic debridement rather than choosing one or the other [15][16][17].
Which topical agents and growth factors improve healing rates?
Autologous platelet-rich plasma and topical platelet-derived growth factor have demonstrated both an increased and faster rate of healing in diabetic foot ulcers compared to placebo [18][19]. There are different types of topical growth factor therapies, including both autogenous and platelet-derived. Autologous platelet-rich plasma mimics the natural healing process [18]. Topical platelet-derived growth factor is also available commercially. Other topical agents are available mostly in the form of antimicrobials. Silver has traditionally enjoyed a high rate of utilization, but, recently, clinically relevant silver resistance has been identified [20]. This realization should play a role in conscientious dressing selections that not only protect the patient being treated but also protect the community.
Which surgical dressings offer the highest probability of healing?
Hydrocolloid-matrix was shown in a systemic review to have the highest probability to offer the best chance of healing diabetic foot ulcers [20]. The decision regarding what to dress an ulcer with should be rooted in science. Among many dressings, options include alginates, foam, hydrocolloids, hydrogels, silver, and collagen. Interestingly, more expensive dressings may offer no advantage over less expensive dressings [21].
How does negative pressure wound therapy facilitate ulcer healing?
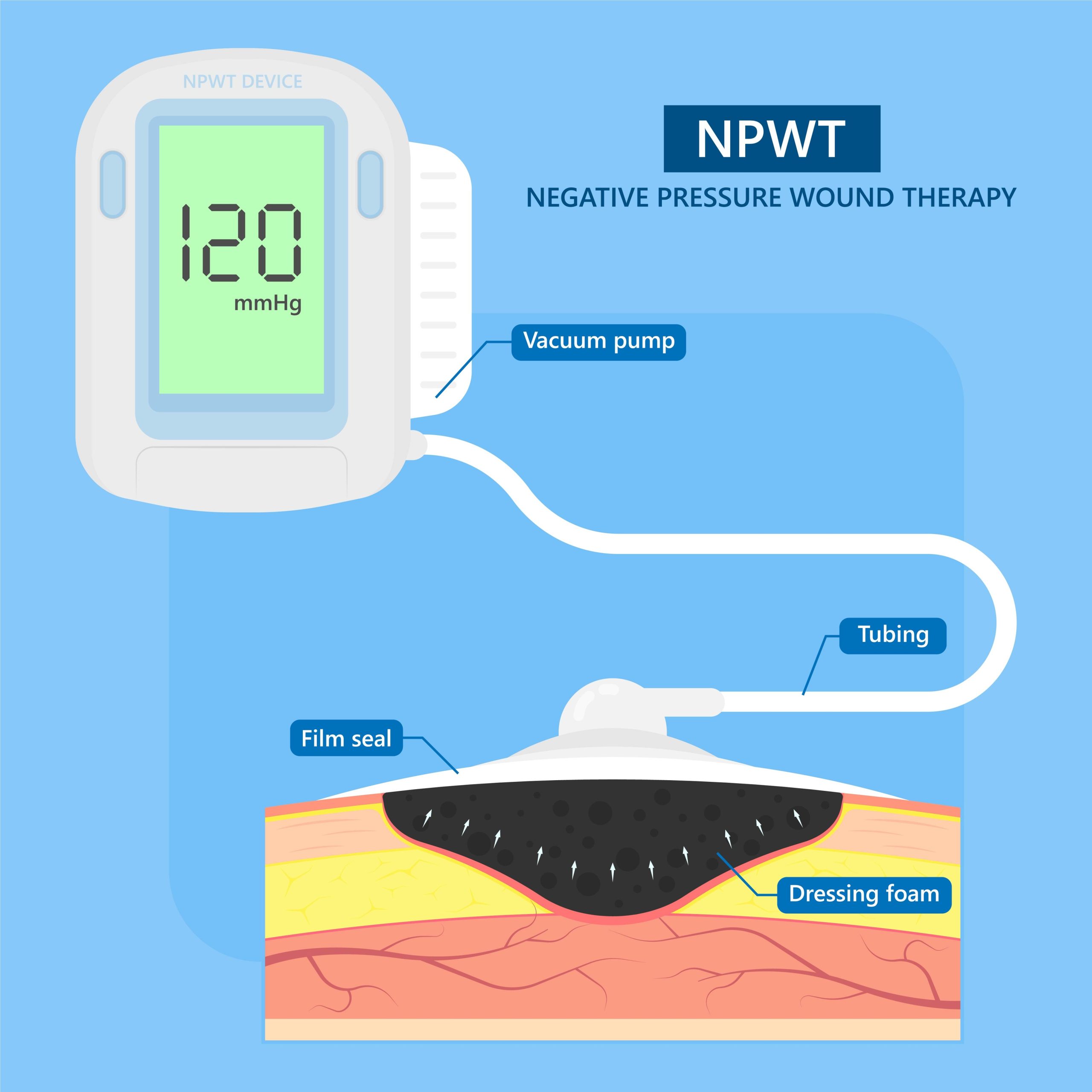 Negative pressure wound therapy delivers sub atmospheric pressure to the ulcer bed and vacuum-assisted drainage, which facilitates the removal of microorganisms, debris, and other unwanted components that can delay healing. Negative pressure wound therapy contributes to the removal of interstitial fluid and a decrease in edema, which increases capillary exchange and allows for improved perfusion and delivery of oxygen and growth factors needed for healing. Negative pressure wound therapy is available in both disposable and non-disposable forms.
Negative pressure wound therapy delivers sub atmospheric pressure to the ulcer bed and vacuum-assisted drainage, which facilitates the removal of microorganisms, debris, and other unwanted components that can delay healing. Negative pressure wound therapy contributes to the removal of interstitial fluid and a decrease in edema, which increases capillary exchange and allows for improved perfusion and delivery of oxygen and growth factors needed for healing. Negative pressure wound therapy is available in both disposable and non-disposable forms.
Decisions regarding pressure settings is an area where standard of care is not always consistent with best practices. A critical decision for most negative pressure wound therapy types is the pressure mode (continuous, intermittent, and variable). Studies show a higher degree of granulation under intermittent and variable pressure than under continuous pressure [22]. While the typical pressure range is between 50 and 150 mmHg, higher pressures should be used when there is more exudate and when a bridge dressing is used [23].
When should skin substitutes and grafts be considered for diabetic foot ulcers?
Graft options for chronic ulcers include both autologous grafts and skin substitute grafts. While autologous grafts are normally preferred over any other option as far as effectiveness, skin substitute options (xenografts, synthetic bilayers, allogenic epidermal or dermal substitutes, composite allografts, allograft placental tissue, allograft human skin cells, and autologous cultured skin) may be considered when they are not available. It is critical to note that in a Cochrane review of seventeen studies regarding the use of skin grafts and tissue replacement products for diabetic foot ulcers, no evidence was found that allows for the recommendation of one type of skin graft or tissue replacement product over another [24]. This same Cochrane paper concluded that while skin grafts and tissue replacements increase the healing rate of foot ulcers, evidence of long-term effectiveness is absent and there is no certainty of cost-effectiveness [24].
Why is graduated compression mandatory for venous leg ulcers?
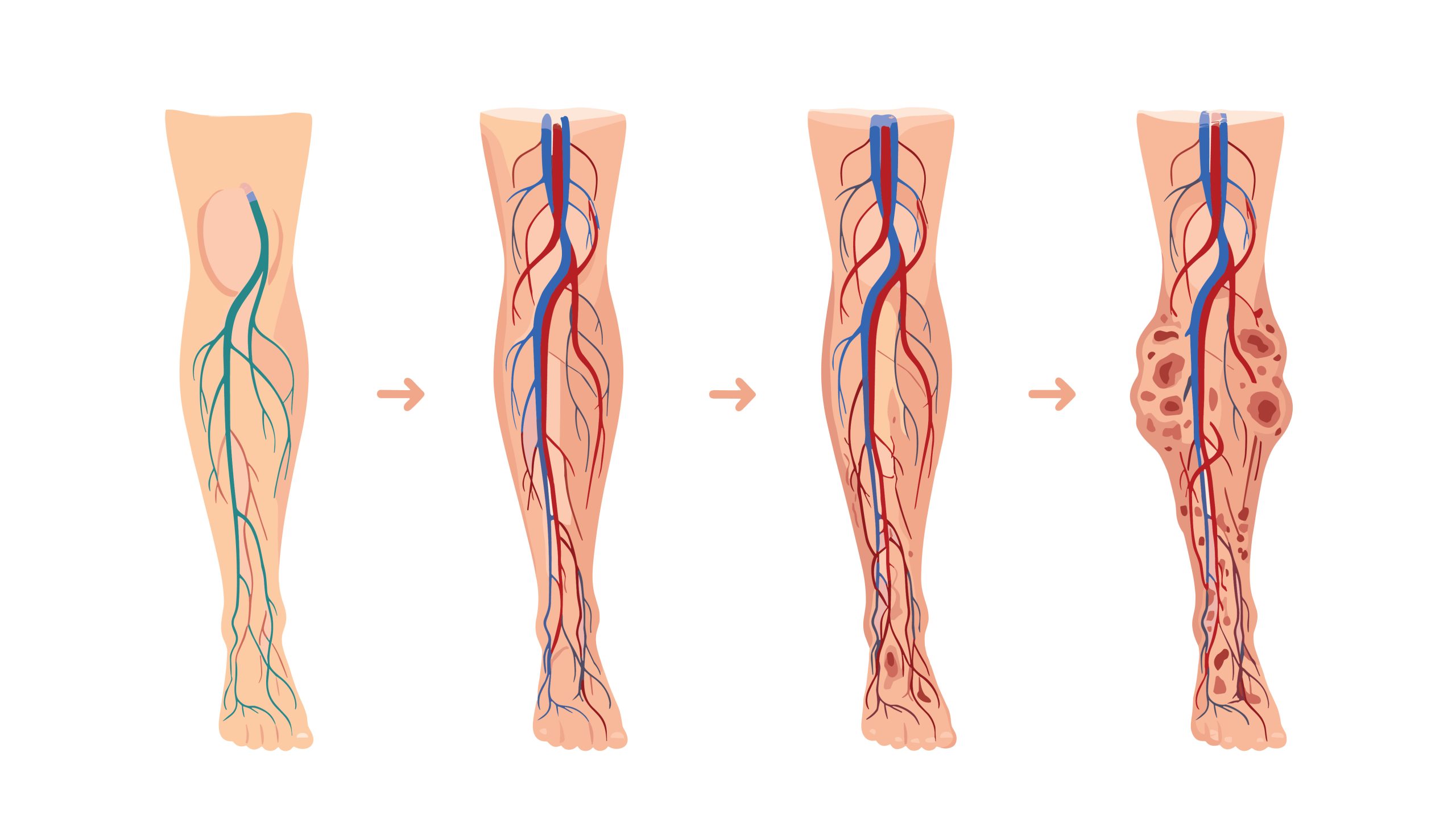 Evidence-based treatment of venous leg disease and venous leg ulcers mandates the use of compression when indicated [25]. However, just employing any type of compression may not be sufficient. It must be graduated, consistent compression at an adequate level. The initial pressure required to collapse a vessel is 30-40 mmHg [26]; therefore, therapeutic compression should achieve at least this degree of pressure. Too often prescription or purchase of inadequate compression options leads to undesirable results. In many cases, healing venous leg ulcers is easier than preventing their recurrence. Adequate below-knee graduated compression stockings or hosiery that patients can tolerate and use as indicated are likely to prevent recurrence of venous leg ulcers [27]. It is incumbent on the prescriber to find a compression option that provides an adequate degree of compression that the patient can actually tolerate. Using compression with a lower degree of pressure often results in poor outcomes. Class III compression provides 25-35 mmHg and using anything less compromises the chances of actually preventing recurrence.
Evidence-based treatment of venous leg disease and venous leg ulcers mandates the use of compression when indicated [25]. However, just employing any type of compression may not be sufficient. It must be graduated, consistent compression at an adequate level. The initial pressure required to collapse a vessel is 30-40 mmHg [26]; therefore, therapeutic compression should achieve at least this degree of pressure. Too often prescription or purchase of inadequate compression options leads to undesirable results. In many cases, healing venous leg ulcers is easier than preventing their recurrence. Adequate below-knee graduated compression stockings or hosiery that patients can tolerate and use as indicated are likely to prevent recurrence of venous leg ulcers [27]. It is incumbent on the prescriber to find a compression option that provides an adequate degree of compression that the patient can actually tolerate. Using compression with a lower degree of pressure often results in poor outcomes. Class III compression provides 25-35 mmHg and using anything less compromises the chances of actually preventing recurrence.
Does Hyperbaric Oxygen Therapy benefit the healing process of chronic ulcers?
Healing processes of chronic ulcers have been shown to accelerate under the influence of hyperbaric oxygen [28]. Hyperbaric medicine involves exposing a patient to hyperbaric oxygen, 100% oxygen at a pressure that is greater than normal. Although controversial in some circles, the evidence-based outlook on the use of hyperbaric medicine for chronic ulcers is simply stated: processes have been clinically shown to accelerate healing [28].
Author: Dr. Jeffrey D. Lehrman, DPM, FASPS, MAPWCA, CPC, CPMA
Co-Authors: Joshua Trujillo, Katelyn Norkowski
Clinical References:
[1] Papanas N, et al. Drug Saf. 2010;33:455-461. [2] Hess, C. Advances in Skin & Wound Care August 2009 – Volume 22 – Issue 9 [3] Sheehan, et al. Diabetes Care 2003 Jun;26(6): 1879-82 [4] Horn SD, et al. Wound Repair Regen 2013 Nov-Dec; 21(6):823-32. [5] Frank, C, et al. Can Fam Physician 2005 Oct 10; 51(10): 1352 – 1359 [6] Kallstrom, G J Clin Microbiol 2014 Aug; 52(8): 2753-2756 [7] Frantz, Rita A. Nursing 2005 July 2005 – Volume 35 – Issue 7 – p 73 [8] Nabuurs-Franssen, MH. Diabetes Care 2005 Feb;28(2):243-7 [9] Health Quality Ontario Our Health Technol Assess Ser 2017; 17(12): 1-124 [10] Armstrong et al. Diabetes Care 2003 Sep:26(9): 2595-7 [11] Association for the Advancement of Wound Care 2010 Guideline of Pressure Ulcer Guidelines; p 9 [12] Wilcox, JR et al. JAMA Dermatol 2013 Sep; 149(9); 1050-8 [13] Carpenter S, et al. WOUNDS 2016;(28)(6Suppl);S1 – S20 [14] Wolcott, RD et al. J Wound Care 2010;19(8);320-328 [15] Motley TA, et al WOUNDS 2014;26: 57-64 [16] Jiminez JC, et al WOUNDS 2017;29:133-139 [17] Tallis A, et al. Clin Ther. 2013;35: 1805 – 1820 [18] Lacci, Kathleen M. et al. Yale J Biol Med. 2010 Mar; 83(1): 1-9 [19] Wieman, TJ, et al. Diabetes Care. 1998;21: 822-827 [20] Finley, Phillip J. Antimicrob Agents Chemother. 2015 Aug; 59(8): 4734-4741 [21] Dumville, JC, et al. Diabetologia. 2012 Jul; 55(7): 1902-1910 [22] Malmsjö M, et al. Eplasty. 2012; 12():e5 [23] Borgquist O, et al. Plast Reconstr Surg. 2011 Feb; 127(2):551-9 [24] Santema TB, et al. Cochrane Database of Systemic Reviews 2016, Issue 2 Art. No. CD011255 [25] Dogra S, et al. Indian Dermatol Online J. 2014 Jul-Sep; 5(3): 400-407 [26] Hegarty M,: Today’s Wound Clinic Oct 10, 2010 vol 5 [27] Nelson EA, et al. Cochrane Database Syst Rev 2000;(4):CD002303 [28] Opasanon S, et al. J Am Coll Clin Wound Spec. 2014 Apr; 6(1-2): 9-13

Dr. Jeffrey D. Lehrman, DPM, FASPS, MAPWCA, CPC, CPMA
Dr. Lehrman is a podiatrist practicing in Fort Collins, CO and operates Lehrman Consulting, LLC which provides consultation services regarding coding, compliance and documentation. Dr. Lehrman is a Certified Professional Coder and Certified Professional Medical Auditor. He serves as a staff liaison at the AMA CPT® Editorial Panel meetings where CPT codes are created, edited, and deleted. He is a Diplomate of the American Board of Foot and Ankle Surgery, Fellow of the American Society of Podiatric Surgeons, and is recognized as a “Master” by the American Professional Wound Care Association. Dr Lehrman is a Fellow of the American Academy of Podiatric Practice Management, Past Director of the American Professional Wound Care Association Board of Directors, and is a Past Chairman of the Board of the American Society of Podiatric Surgeons. Dr. Lehrman is also on the editorial advisory board of the journal WOUNDS.




{kind=link}
{kind=link}
{kind=link}
{kind=link}